
Basal thumb arthritis is a very common condition mainly affecting middle aged women but also men who perform manual tasks. It presents with pain at the base of the thumb and difficultywith everyday tasks such as opening tight jar lids, pain on wringing out a cloth and difficulty holding objects such as a kettle.
The condition is confirmed by expert examination – pain and crepitus on grinding or axially loading the thumb. As the disease progresses the hand can adopt a characteristic appearance as the basal thumb joint gradually subluxes and the thumb adducts with secondary compensatory hyperextension at the metacarpophalangeal joint resulting in a Z thumb deformity in advanced cases.

XRs will usually confirm the diagnosis. Occasionally, the XRs will show that the at the joint below (the scaphotrapeziotrapezoidal joint,STTJ ) is also arthritic.
Treatment is tailored to the severity of disease. In mild cases lifestyle modification, simple analgesia and possible splintage may suffice. In others, a steroid injection into the basal thumb joint can be helpful. In fact the majority of patients who get as far as presenting to a hand surgeon will probably have a steroid injection as most will have already tried the simpler treatments. The risks of steroid injections are post-steroid flare, depigmentation and skin atrophy. Yours surgeon will discuss these with you.
Surgery when all other treatments have failed
There are 2 surgical options for base of thumb arthritis – trapeziectomy (and LRTI – ligament reconstruction tendon interposition) or the newer joint replacement (MAIA) . The jury is out as to which is best but there are differences in the technical procedure , risks , rehabilitation on and benefits It is important that the surgeon discusses both options with the patient ,
Overview
The trapeziometacarpal joint, located at the base of the thumb, is commonly affected by osteoarthritis, causing pain, stiffness, and reduced function. Surgery is considered when non-surgical treatments (e.g., splints, injections, therapy) fail to relieve symptoms. Two common procedures are:
Trapeziometacarpal Joint Replacement
Description:
The damaged TMC joint surfaces are removed, and an artificial joint (prosthesis) is implanted. The prosthesis typically consists of a metal stem in the metacarpal and a socket component replacing the trapezium.
Anaesthesia: General or regional (nerve block which makes the arm numb).
-Duration: Approximately 1–1.5 hours.
-Hospital Stay: Usually same-day discharge
Rehabilitation
-Immobilization: A splint is worn for 2–4 weeks to protect the implant.
– Exercises: begin 2 weeks post-surgery, focusing on:
– Restoring thumb motion and strength.
– Preventing stiffness.
– Gradual return to daily activities.
– Recovery Timeline:
– Light activities (e.g., writing): 2-6 weeks.
– Full strength and heavy tasks: 6weeks to 3 months.
– Follow-Up: Check at 4-6 weeks monitor implant stability and ensure function improving.
Risks
– Implant-Related:
– Loosening or wear of the prosthesis over time (may require revision surgery).
– Dislocation of the implant.
– Fracture during implantation may require conversion to trapeziectomy
– General Surgical Risks:
– Infection (1–2% risk).
– Nerve or blood vessel injury (rare).
– Persistent pain or stiffness.
– Long-Term: Studies currently show that approximately 85-90% of implants are still functioning well after 12 years. There is a risk of needing further surgery at a later date.
Benefits
– Pain Relief: Significant reduction in thumb pain.
– Function: Improved thumb motion and grip strength compared to trapeziectomy in some studies.
– Stability: Maintains thumb length and alignment, potentially reducing deformity.
– Recovery: Potentially faster return to function than trapeziectomy due to preserved joint structure.
Trapeziectomy (with or without Ligament Reconstruction and Tendon Interposition – LRTI)
Procedure
– Description: The trapezium bone is removed, creating a space at the thumb base so that the worn joint surfaces do not rub against each other. In LRTI, a tendon (often from the wrist) is used to stabilize the joint and fill the space.
– Anaesthesia: General or regional.
– Duration: 1–1.5 hours.
– Hospital Stay: Typically discharge same day
Rehabilitation
-Immobilization: A splint is worn for 4–6 weeks.
– Therapy: Hand therapy starts 4–8 weeks post-surgery, focusing on:
– Restoring thumb mobility and strength.
– Preventing scar tissue formation.
– Recovery Timeline:
– Light activities: 8–12 weeks.
– Full strength: 6–12 months (longer than joint replacement).
– Follow-Up: Monitoring for thumb stability and function.
Risks
– Procedure-Specific:
– Thumb weakness due to loss of trapezium (may affect pinch strength).
– Instability or collapse of the thumb base (metacarpal subsidence).
– 5-10% of individuals unhappy with level of improvement
– General Surgical Risks:
– Infection (1–2% risk).
– Nerve or tendon injury.
– Complex regional pain syndrome (rare).
– Long-Term: No implant, so no risk of implant failure, but thumb shortening may occur.
Benefits
-Pain Relief: Effective long-term pain reduction in most patients.
– Durability: No prosthesis, so no need for revision due to implant wear.
– Proven Track Record: Widely performed with reliable outcomes over decades.
– Suitability: Ideal for older or less active patients, as it avoids implant-related complications.
Comparison
| Joint Replacement | Trapeziectomy | |
| Procedure | Replaces joint with prosthesis | Removes trapezium; may use tendon for stability |
| Pain Relief | Excellent in most cases | Excellent in most cases |
| Thumb Strength | Often better pinch/grip strength initially | May have reduced pinch strength long-term |
| Thumb Stability | Maintains thumb length and alignment | Risk of thumb shortening or instability |
| Recovery Time | Faster return to function (2-4 months) | Slower, full strength may take 6–12 months |
| Longevity | Implant may wear out unknown very long term outcome | No implant, so no wear; lifelong durability |
| Risks | Implant loosening, dislocation, revision surgery | Weakness, instability, thumb collapse |
| Ideal Candidate | Younger, active patients needing strength. Little or no arthritis in joint below. | Older or less active patients |
Additional Information
– Non-Surgical Alternatives: Before surgery, consider splints, physical therapy, or corticosteroid injections. These may delay or avoid the need for surgery.
– Post-Surgery Care: Follow your surgeon’s and therapist’s instructions to optimize recovery and minimize complications.
– Questions for Your Surgeon:
– Which procedure is would you recommend for my specific condition?
– What is the expected recovery timeline for my lifestyle?
– How many of these procedures have you performed?
This is entrapment of the ulnar nerve at the level of the medial epicondyle of the elbow (‘funny bone’) and is characterised by numbness of the little and ring fingers, tingling, weakness and wasting of the small muscles of the hand, depending on the severity. The cause is usually not usually obvious; occasionally it develops in patients who lean on their elbows a lot, have had trauma to the elbow or who have arthritis.
Diagnosis and Treatment
This is usually confirmed with nerve conduction studies. Treatment if mild, may simply involve lifestyle modifications (avoiding sleeping with elbows bent/avoidance of leaning on elbows) or in patients with significant symptoms, surgical decompression of the ulnar nerve at the level of the ‘funny bone’.
In mild/moderate cases the sensory symptoms often resolve with surgery but in advanced cases, the aim of surgery is to prevent further damage to the nerve.

Named after the Swiss Surgeon De Quervain who originally described this painful condition as ‘washerwoman’s sprain’ and by described rather unflatteringly by Finkelstein as a condition affecting the ‘labouring classes’!
De Quervain’s syndrome is characterised by pain and swelling on the radial aspect of the wrist with painful thumb movements and weakness in grip. There is a fairly strongassociation with pregnancy and the post-partum period – it is likely that this is due to hormonal and fluid changes.
The pain results from degenerative changes affecting the strap like tunnel around the tendons on the radial aspect of the wrist. The tunnel narrows and constricts (hence the condition is sometimes called stenosing tenosynovitis) and as a result the tendons fail to glide normally resulting in pain and swelling.
Mild cases may settle without any treatment. Sometimes a splint will suffice. In the more symptomatic, a steroid injection into the painful area will have a 70-80% success rate. The side effect of steroids are depigmentation and skin changes which your surgeon will discuss with you.
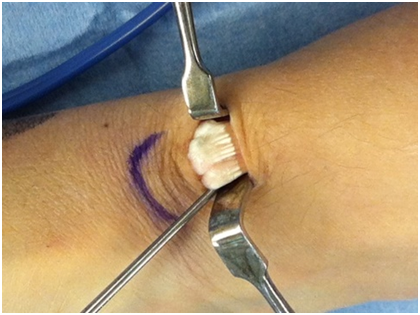
Surgical decompression of the tunnel (s) around the tendons is offered in when symptoms do not settle. This is performed under regional or general anaesthesia, via a tranverse incision under loupe magnification protecting the nerve branches. The sheath surrounding the tendons to released so that the tendons can glide freely. Your surgeon will discuss this with you in greater detail.
Named after the French Napoleonic Surgeon Baron Dupuytren, this is a common condition affecting the hand characterised by nodules or cords starting in the palm. In a third of patients the nodules will progress into cords which can cause digital contracture. The little and ring fingers are most affected. The aggressive form of Dupuytren’s, is characterised by radial (thumb and index) sided disease,bilaterality, ectopic disease (eg in the feet) and early age onset and strong family history.
The cause is unknown but we know that there is a genetic predisposition and people of Northern European (‘Viking’) heritage are particularly affected. It was previously thought to be associated with the ’good life’ (heavy smoking and alcohol consumption) but there is not enough evidence to back this up. There is an association with diabetes. Trauma /injury can accelerate the onset.

If function is unaffected then no treatment is necessarily required. The interventional options are:
Xiapex (collagenase) injections – depending on disease severity
Needle fasciotomy
Selective fasciectomy
Total fasciectomy
Dermofasciectomy (usually in the revision setting)- skin grafting
The available evidence does not support the use of radiotherapy for Dupuytren’s. Surgery is usually followed with splintage and hand therapy.
Consent information for surgery for Dupuytren’s
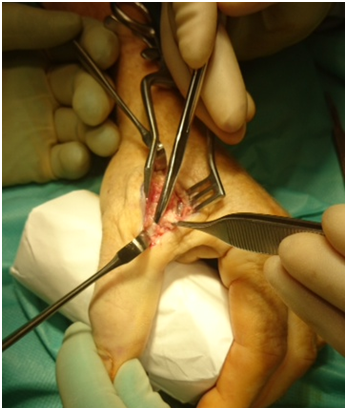
This involves an anaesthetic – regional ‘wide awake’ (whole arm numbed by an anaesthetist) or General Anaesthetic depending on patient preference. Usually day surgery. An extensive dissection is performed in order to identify and remove as much diseased tissue as possible and to visualise and protect the neurovascular (nerves/blood vessels) bundles. Post-operative elevation for a few days is required, plaster removal and splint application at 1 week, Hand Therapy to commence (and splint) at 1week post -op, wound check and removal of sutures 2 weeks. Hand therapy is an important component of treatment post-operatively and is required for several weeks/months depending on severity of disease.

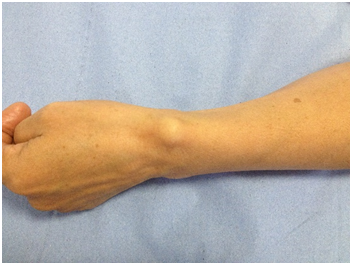
These are common fluid filled sacs presenting as swelling around joints or tendons, typically on the back of the wrist, near the ends of fingers (mucous cysts or pearl ganglia) or at the front of the wrist. The cause is usually unknown and several theories are postulated including wear and tear of the underlying joint or tendon resulting in synovial or joint fluid leaking out presenting as a swelling.
Ganglia may or may not be painful. They can become bigger or smaller and can disappear with time.
If the ganglion is not painful then reassurance and confirmation of the diagnosis is all that is required. If symptomatic then the first line treatment is needle aspiration, or steroid injection which has a 50% success rate.
Surgery is offered if the ganglion is persistently painful despite aspiration.



This is a common hand condition characterised by pain and clicking of the digit. Sometimes the finger gets stuck in the palm (locking) and the patient has to pull it straight. The cause is related to degenerative change in part of the palmar pulley system which undergoes wear and tear thus narrowing. As a result the tendon fails to slide smoothly in it’s tunnel; instead triggering or locking occurs
Patients with diabetes are frequently affected but it is important to note that most patients with triggering are not diabetic.
Steroid injections into the palm around the pulley has a success rate of 70-80 %. This is lower for diabetics.
If steroid injections fail then surgical decompression is offered. This involves a small cut in the palm and release of the pulley at the mouth of the tendon sheath. A light dressing is applied to the wound for 10-14 days and the hand is initially elevated whilst maintaining good finger movements.



A hyperextension injury of thumb can result in an ulnar collateral ligament (UCL) injury. The UCL is a stout, thick and strong ligament on the inside of the thumb at the level of the metacarpophalangeal joint. It is essential for the stability and patients who have completely ruptured this will notice instability on key grip pinch. It can be quite debilitating and depending on the degree of rupture surgery may be advised.
If the UCL is partially sprained or damaged, it may be successfully treated with splint immobilisation. However a completely ruptured UCL may well required surgical repair. The anatomy is such that is possible for the ligament to rupture and each end of the ligament end up on either side of a covering fascial structure known as the adductor aponeurosis resulting in what is called a Stena lesion – in this situation , the UCL will never heal well and surgery is usually recommended.
Sometimes the UCL is avulsed taking a bony fragment with it. If the bony fragment is displaced away form it’s origin then the bony fragment is fixed back onto it’ s origin.
After surgical repair, splintage and hand therapy is often required.
In the unusual situation of a delay in treatment foran ulnar collateral ligament rupture (beyond weeks/months), direct repair may not be possible and sometimes a reconstruction of the ligament using a tendon free graft is performed.


There is a lot of interest in the relatively new and emerging area of biologics – platelet rich protein (PRP). It has been made ‘fashionable‘ by the likes of Rafael Nadal and Tiger Woods. The healing of damaged, injured or inflamed tissues involves a complex inflammatory / healing response. Platelets release growth factors at the injured site and these are involved in the healing response. PRP is a high concentration of platelets and therefore growth factors which are involved in the healing response.
What is PRP?
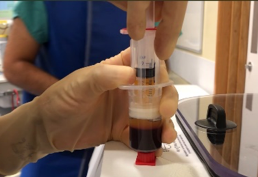
PRP is obtained from the patient by taking a sample of their blood, spinning it down in a centrifuge machine which separates the blood into various components – red cells, white cells and the plasma rich layer. The latter is taken and injected into the patient’s injured region. It contains a high concentration of active platelets which release growth factors involved in the healing of damaged tissues – tendons, ligaments, joints (including degenerative or arthritic joints).
Sample of blood taken from patient
Centrifugation separates blood into different components
PRP (top layer) is taken and injected into damaged tissue
Benefits
The main advantage is that the substance injected is from the patient him/herself so there is a negligible risk of any adverse reaction. It is only as invasive as having a blood test and is a fairly quick procedure done in the outpatient setting usually.
Studies have confirmed the effectiveness of PRP for tennis elbow, jumper’s knee, plantar fasciitis and osteoarthritis of the knee. Studies around the hand and wrist do exist but it is not as well established.