
Scaphoid fractures are the commonest carpal fracture yet a potentially serious injury resulting in considerable disability (non-union / arthritis) if inadequately treated. Scaphoid fractures are commonly missed partly because the clinical signs are often unimpressive and 25 % of initial XRs will fail to show a scaphoid fracture when there is one. The scaphoid has a poor blood supply which is why even in fit and healthy patients it sometimes fails to heal. Smoking is considered a poor prognostic factor for scaphoid union.
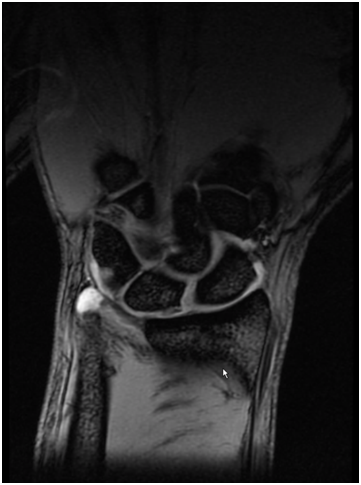
If a scaphoid fracture is suspected an MRI scan may be necessary (advised by NICE guidelines) to confirm if X-rays are not 100% diagnostic.
The treatment of a scaphoid fracture depends on the personality of the fracture: displaced, undisplaced, proximal pole vs distal pole vs waist fracture. Your surgeon will discuss the different types with you.
A completely undisplaced scaphoid fracture (difficult to see on XR) can be treated with good success in a plaster. This plaster does not need to include the thumb but the average time in plaster is between 8-12 weeks.
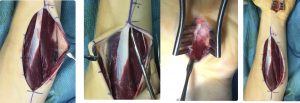
A displaced fracture has a significantly lower union rate and so in these cases surgery may be offered. Surgery is also offered for proximal pole fractures because the blood supply in this region is poor and thence the union rates lower. Surgery will entail a general or a regional anaesthetic (wide awake surgery with numbed arm), and then a screw is passed and buried within the substance of the scaphoid.
There is a period of immobilisation thereafter but less than with non-operative treatment. Surgery has a few risks and does not guarantee union. When patients present late with a scaphoid that has not united then it is often necessary to use bone graft (taken from pelvis or back of wrist) as well as screw fixation. Your surgeon will discuss this with you.




Surgery involves arthroscopic (keyhole) assessment and subsequent repair. This will involve a small incision (not keyhole) on the ulnar side of the wrist and repair using an anchor suture (metallic stud buried in the bone). Post-operatively an above elbow splint is applied for a total of 6 weeks. Your surgeon will discuss this with you.
A hyperextension injury of thumb can result in an ulnar collateral ligament (UCL) injury. The UCL is a stout, thick and strong ligament on the inside of the thumb at the level of the metacarpophalangeal joint. It is essential for the stability and patients who have completely ruptured this will notice instability on key grip pinch. It can be quite debilitating and depending on the degree of rupture surgery may be advised.
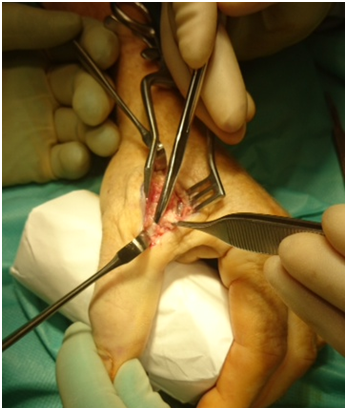
If the UCL is partially sprained or damaged, it may be successfully treated with splint immobilisation. However a completely ruptured UCL may well required surgical repair. The anatomy is such that is possible for the ligament to rupture and each end of the ligament end up on either side of a covering fascial structure known as the adductor aponeurosis resulting in what is called a Stena lesion – in this situation , the UCL will never heal well and surgery is usually recommended.
Sometimes the UCL is avulsed taking a bony fragment with it. If the bony fragment is displaced away form it’s origin then the bony fragment is fixed back onto it’ s origin.
After surgical repair, splintage and hand therapy is often required.
In the unusual situation of a delay in treatment foran ulnar collateral ligament rupture (beyond weeks/months), direct repair may not be possible and sometimes a reconstruction of the ligament using a tendon free graft is performed.


After all non-operative options are exhausted Total Wrist Fusion or Total Wrist Replacement can be considered can be considered.
This is fairly common and result from general wear /tear and aging or secondary to trauma ie post traumatic.
Typically this presents with pain, swelling and stiffness. Sometimes the wrist feels weak and the patient struggles to carry heavy objects or load the wrist.
Treatment depends on severity of disease. In mild cases simple lifestyle modification, anti-inflammatories (both tablet and ointment) and splints might prove helpful. Steroid injections can also have a powerful effect in moderate cases. If all conservative measures fail then surgery may be appropriate including total wrist replacement or fusion. There are a range of lesser operations which are designed to maintain some movement as well as address pain.
Miss Umarji recently performed the first Total Wrist Replacement at St George’s NHS Trust

After years of pain patient Julie Richardson was delighted to be the forst patient to have a Total Wrist Replacement at St George’s London.

These injuries are relatively common and are either frequently missed or underestimated. The scapholunate ligament (SLL) is a ligament in the central aspect of the wrist and is an important stabiliser of the wrist . It is therefore the equivalent of the “Cruciate” ligament of ACL of the knee. If it is seriously injured the patient can develop pain on load bearing esp doing press ups or lifting objects. Certain everyday tasks can become painful if seriously injured. If the injury is neglected, premature arthritis and collapse of the wrist may occur in certain situations.
After scaphoid fractures, the SLL is probably the most commonly missed injury and this can have potentially detrimental effects for the patient.
An early MRI scan is required to make a prompt diagnosis. If diagnosed early (within 6 weeks) a repair of the ligament is possible. When diagnosed later, reconstruction using tendon graft is often required. The latter is more complex surgery and therefore an early diagnosis is recommended.
Surgery is usually followed by 6 weeks of splintage to protect the repair. Intensive rehabilitation and hand therapy is required afterwards to regain strength and movement. It takes several months to feel the benefit of surgery.
The procedure technically demanding and so it is essential that your surgeon is an expert on this type of surgery.

Consent information for wrist fracture surgery
This is a common injury resulting from a fall onto an outstretched hand. It can often occur as a result of low energy trauma in the elderly and higher energy injuries are seen in the younger population. The treatment can be operative (surgical fixation) and non-operative (treatment in plaster) depending on the type of fracture. Your surgeon will advise on the type of treatment of your fracture.


Surgical fixation can take the form of plating the wrist. This will involve an incision on the palmer side of the wrist, putting the fragments of bone back in the right place and then holding them in place with a plate. This allows earlier mobilisation of the wrist (less time in plaster). There are surgical risks which your surgeon will discuss with you and sometimes (but not always) it is necessary to remove the plate at a future date.
The main advantage of treatment in plaster is that there is no surgical risk. However this is not suitable for all as the broken fragments of bone need to be well aligned. A degree of malunion may result. Your consultant will discuss suitable treatment options with you fully.


This unusual but very real condition typically affects elite rowers , those involved in motocross as well as other high intensity sportsmen and women . It is characterised by intense pain , deadness, cramping , swelling of forearms and tenseness in the forearms. Physical enlargement as well as ‘hardness’ of the forearms is frequently described. It occurs predictably after a period of intense activity and is very debilitating. The oarsman or motorcyclist is often unable to continue and has to rest / abstain.
Diagnosis and investigations .
Diagnosis can be tricky but it is made largely on the symptoms and presentation . The investigations are not always helpful but it is important to exclude other causes of similar symptoms . MRI and nerve conduction studies are helpful in particular. It is difficult to re-create the symptoms so the investigations can be normal.
Management including surgery.
Initially non-operative treatments such as rest, activity modification , physiotherapy , icing , massage are all tried extensively. If these techniques do not help and the symptoms are debilitating then surgical decompression is considered.this involves full release of all affected compartments as well as potential decompression of nerves .
Miss Umarji First Total Wrist Replacement at St George’s Hospital
After all non-operative options are exhausted Total Wrist Fusion or Total Wrist Replacement can be considered.
This is fairly common and result from general wear /tear and aging or secondary to trauma ie post traumatic.
Typically this presents with pain, swelling and stiffness. Sometimes the wrist feels weak and the patient struggles to carry heavy objects or load the wrist.
Treatment depends on severity of disease. In mild cases simple lifestyle modification, anti-inflammatories (both tablet and ointment) and splints might prove helpful. Steroid injections can also have a powerful effect in moderate cases. If all conservative measures fail then surgery may be appropriate including total wrist replacement or fusion. There are a range of lesser operations which are designed to maintain some movement as well as address pain.
Miss Umarji recently performed the first Total Wrist Replacement at St George’s NHS Trust
After years of pain patient Julie Richardson was delighted to be the forst patient to have a Total Wrist Replacement at St George’s London.

There is a lot of interest in the relatively new and emerging area of biologics – plasma rich protein (PRP). It has been made ‘fashionable‘ by the likes of Rafael Nadal and Tiger Woods. The healing of damaged, injured or inflamed tissues involves a complex inflammatory / healing response. Platelets release growth factors at the injured site and these are involved in the healing response. PRP is a high concentration of platelets and therefore growth factors which are involved in the healing response.
What is PRP?
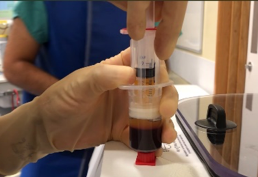
PRP is obtained from the patient by taking a sample of their blood, spinning it down in a centrifuge machine which separates the blood into various components – red cells, white cells and the plasma rich layer. The latter is taken and injected into the patient’s injured region. It contains a high concentration of active platelets which release growth factors involved in the healing of damaged tissues – tendons, ligaments, joints (including degenerative or arthritic joints).
Sample of blood taken from patient
Centrifugation separates blood into different components
PRP (top layer) is taken and injected into damaged tissue
Benefits
The main advantage is that the substance injected is from the patient him/herself so there is a negligible risk of any adverse reaction. It is only as invasive as having a blood test and is a fairly quick procedure done in the outpatient setting usually.
Studies have confirmed the effectiveness of PRP for tennis elbow, jumper’s knee, plantar fasciitis and osteoarthritis of the knee. Studies around the hand and wrist do exist but it is not as well established. Miss Umarji is currently the Chief Investigator for a major study looking at the effectiveness of PRP for base of thumb arthritis.
In select cases surgery can potentially be avoided if PRP is successful.